Erectile Dysfunction and Treatment After Radical Prostatectomy
Radical prostatectomy (RP) is one of the common treatment methods for localized prostate cancer, performed with open, laparoscopic or robotic-assisted techniques. However, one of the most important postoperative complications, erectile dysfunction (ED), can negatively affect the quality of life of patients. In this article, the preservation and recovery of erectile function after different surgical approaches will be examined and important factors such as nerve preservation, surgical expertise and rehabilitation strategies will be discussed.
How common is ED after RP?
The prevalence of erectile dysfunction (ED) after radical prostatectomy varies depending on variables such as surgical technique, nerve-sparing methods, and patient factors (age, preoperative erectile function).
ED Prevalence According to Surgical Approach
- Open Radical Prostatectomy (ORP): ED rates range from 60% to 90%, and recovery can take 2–3 years when nerve-sparing techniques are used.
- Laparoscopic Radical Prostatectomy (LRP): Similar to ORP, ED rates range from 50% to 85%. Some studies report slightly better results because of less blood loss and better visualization.
- Robotic Assisted Radical Prostatectomy (RARP): ED rates range from 30% to 80%, with faster recovery due to better application of nerve-sparing techniques and increased surgical precision.
What are the main factors that affect the occurrence of ED?
Some important risk factors that affect the development of ED after radical prostatectomy are:
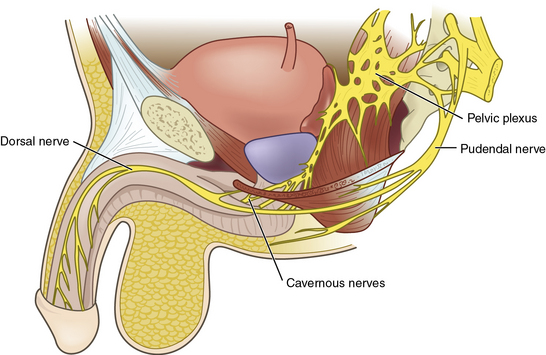
- Nerve-sparing Surgery: Bilateral nerve-sparing techniques significantly increase the likelihood of recovery of erectile function.
- Surgeon Experience: Surgeons with higher patient volumes tend to achieve better functional outcomes.
- Patient Age & Preoperative Function: Young patients and those with good erectile function before surgery have an advantage in terms of recovery.
- Post-Operative Rehabilitation: The use of phosphodiesterase type 5 (PDE5) inhibitors, vacuum erection devices, and penile rehabilitation programs can positively affect the treatment process.
In general, robotic-assisted techniques may offer better results in preserving erectile function, but it should be noted that the risk of ED is not completely eliminated. Therefore, preoperative counseling and rehabilitation strategies are of great importance.
What is the best way to prevent ED after RP?
The best method for preserving erectile function depends on surgical technique, nerve-sparing strategy, and surgeon experience. However, current evidence suggests that robotic-assisted radical prostatectomy (RARP) is the technique that best preserves erectile function.
Comparison of Surgical Methods
| Surgical Method | Erectile Function Preservation Rate | Main Advantages | Main Disadvantages |
| Open Radical Prostatectomy (ORP) | 10–40% (after 1 year) | Experienced surgeons can perform precise nerve preservation; advantage of direct tactile sensation. | Higher risk of nerve damage due to lower magnification. |
| Laparoscopic Radical Prostatectomy (LRP) | 20–50% (after 1 year) | Minimally invasive; better visualization compared to open surgery. | Less range of motion than robotic surgery; steep learning curve. |
| Robotic Assisted Radical Prostatectomy (RARP) | 40–70% (after 1 year) | High precision, 3D magnification imaging, better nerve protection results. Less blood loss and faster recovery process. | Requires special equipment and training; costly. |
Why is ED less common after robotic surgery?
Although no method completely eliminates the risk of ED, robotic-assisted radical prostatectomy (RARP) offers the best results when performed by an experienced surgeon using a bilateral nerve-sparing technique .
- Better Visualization and Precision: Robotic systems provide surgeons with a magnified 3D image so they can better preserve the neurovascular bundles necessary for erection.
- Minimal Tissue Trauma: The precision of robotic arms reduces unnecessary pressure on nerves, reducing the risk of damage.
- Faster Recovery: Studies show that patients who undergo RARP regain erectile function faster compared to open and laparoscopic methods.
- Advanced Nerve-Sparing Techniques: Robotic surgery offers the opportunity to perform nerve dissection more gently, minimizing nerve damage.
Post-RP ED treatment options
There are different treatment options depending on the severity of ED and the nerve protection status:
First Line: PDE5 Inhibitors
- Medications: Sildenafil (Viagra), Tadalafil (Cialis), Vardenafil (Levitra), Avanafil (Stendra)
- Effectiveness: Works better if at least one neurovascular bundle is preserved during surgery.
- Usage: Prescribed in low daily doses or as needed.
- Limitations: May not be effective if nerve damage is severe.
Second Step: Vacuum Erection Devices (VED)
- How It Works: It creates a vacuum around the penis, increasing blood flow.
- Benefits: Maintains the health of penile tissue and prevents fibrosis.
- Limitations: May be an uncomfortable or unnatural experience for some patients.
Third Step: Intracavernous Injections (ICI)
- Medicines: Alprostadil, Trimix (Papaverine + Phentolamine + Alprostadil)
- Effectiveness: Up to 80% success rate; works even when PDE5 inhibitors are ineffective.
- Limitations: Patients must self-inject.
Urethral Suppositories (MUSE – Medical Urethral Erectile System)
• Drug Used: Alprostadil (urethral pellet)
• How Does It Work? Stimulates blood flow when inserted into the urethra.
• Effectiveness: Less effective than injections, but may be helpful for some men.
• Limitations: May cause urethral pain or irritation.
Last Resort: Penile Prosthesis (Prosthesis Surgery)
- Types:
- Inflatable prosthesis: A fluid-filled device that mimics a natural erection.
- Flexible prosthesis: Semi-rigid rods that can be positioned manually.
- Effectiveness: Up to 90% patient satisfaction.
- Limitations: Requires surgery and is irreversible.
Lifestyle Changes and Psychological Support
• Pelvic Floor Therapy: Strengthens the muscles related to erection.
• Regular Exercise: Improves blood circulation and overall health.
• Healthy Nutrition: A heart-healthy diet contributes positively to erectile function.
• Counseling and Sex Therapy: Helps manage anxiety, depression and relationship problems.
Emerging Treatments
• Shock Wave Therapy: Uses low-intensity waves to increase blood flow to the penis (still experimental).
• Stem Cell Therapy and PRP (Platelet-Rich Plasma): Being investigated for nerve regeneration.
What is the most effective method for treating ED after RP?
The most effective method for treating erectile dysfunction (ED) after radical prostatectomy depends on the degree of nerve damage and the individual patient’s response. However, penile implants (prosthetic surgery) are considered the most effective method for patients experiencing severe or persistent ED.
Best Treatment Options Based on ED Severity:
| ED Severity | Recommended Treatment | Effectiveness | Things to Consider |
| Mild to Moderate ED | PDE5 inhibitors (Viagra, Cialis, Levitra) | 50–70% success rate (if nerves are preserved) | It is more effective in patients undergoing nerve-sparing surgery; less effective in cases of severe nerve damage. |
| Medium ED | Vacuum erection device (VED) | 50–60% success rate | Helps maintain penile tissue health; may not feel natural for some men. |
| Moderate to Severe ED | Intracavernous injections (Alprostadil, Trimix) | 80% success rate | It is highly effective even in patients who have not undergone nerve-sparing surgery; it requires injection. |
| Severe/Persistent ED | Penile implants (prosthetic surgery) | 90–95% success rate | The most reliable long-term solution; requires surgery but offers high patient satisfaction. |
Why are penile implants the most effective solution?
For mild to moderate ED, PDE5 inhibitors or injections may be effective, but for severe and persistent ED, penile prosthesis implantation is the most effective and reliable solution.
- High Success and Satisfaction Rate: 90–95% of patients report successful sexual function and high satisfaction.
- Works Independently of Nerve Damage: Unlike PDE5 inhibitors, it does not depend on nerve integrity.
- Permanent and Predictable Results: Provides erections on demand without the need for medication or external devices.
Conclusion
ED is a common complication after radical prostatectomy. RARP offers the best results in preserving erectile function. Treatment options vary depending on the patient’s level of ED, and early rehabilitation and individualized treatment plans can positively impact the recovery process.
Treatment Options:
- First Step: PDE5 inhibitors (Viagra, Cialis) – Effective if nerves are protected. Second Step: Vacuum erection devices (VED) – Help maintain blood flow.
- Third Step: Intracavernous injections (Alprostadil, Trimix) – Has a high success rate even in severe cases.
- Last Resort: Penile implants (prosthetics) – The most effective long-term solution for persistent ED.
Early penile rehabilitation and a personalized treatment plan can contribute to improved erectile function and improved overall quality of life.