


Dr. Sharmila Rathi is a dedicated Pediatrician, Child Specialist, and expert medical author for HealthyPost. Currently serving at the prestigious Grant Government Medical College & Sir JJ Group of Hospitals, Mumbai, she brings extensive clinical experience managing pediatric healthcare challenges at one of India's premier government teaching hospital networks.
Dr. Rathi specializes in neonatal care, childhood developmental milestones, and acute pediatric medical interventions. At HealthyPost, she directly authors and develops highly reliable, evidence-based pediatric health guides, ensuring parents and caregivers receive accurate, actionable, and practical health guidance.
Core Editorial Expertise: Neonatal Care Protocols • Childhood Development Milestones • Pediatric Interventions • Evidence-Based Medical Writing
🩺 Authored & Clinically Vetted by a Pediatric Specialist
Medical Disclaimer: This expert content has been authored and clinically compiled by Dr. Sharmila Rathi (Pediatrics & Child Care, Sir JJ Hospital, Mumbai). The information provided throughout this guide is strictly for educational, informational, and general parental reassurance purposes. It does not constitute formal pediatric medical advice, diagnosis, or treatment for any individual child. Always consult immediately with a qualified pediatrician, healthcare specialist, or your local neonatal care provider regarding persistent infant lip blisters, potential oral infections, or feeding difficulties.
A sucking blister can look alarming the first time a parent spots it on a newborn’s lip. In clinical practice, we often hear the same question: “Is this normal, or is something wrong?” Most of the time, a sucking blister is a harmless friction blister caused by feeding. It may appear after breastfeeding, bottle feeding, or frequent self-soothing on fingers or hands. Still, because it can resemble other mouth problems, parents understandably worry about infection, latch problems, or pain.
This article explains what a newborn sucking blister is, why it forms, how to tell sucking blister vs thrush, when to seek help, and what treatment usually involves. We’ll also look at practical feeding adjustments, including breastfeeding latch technique, and when a newborn lip blister from bottle feeding may deserve a closer look. If your baby also has digestive concerns, parents often explore related newborn health topics such as Undigested Milk in Baby Stool or Blood in Baby Stool while tracking feeding patterns.
1. What is a newborn sucking blister?
A sucking blister is a small blister, thickened patch, or fluid-filled bump that usually appears on a newborn’s upper lip. It develops from repeated friction during sucking. This is why some clinicians also describe it as a neonatal friction blister.
In most cases, it is:
- Benign
- Temporary
- Not contagious
- Not a sign of poor hygiene
- Not usually painful enough to disrupt feeding
The lesion may look clear, yellowish, white, or slightly callused. Some babies are born with one. Others develop it in the first days or weeks of life as the infant sucking reflex friction repeatedly affects the delicate skin of the lip.
Most studies agree that sucking blisters are self-limiting. They often heal without treatment once feeding mechanics improve or as the lip adapts to repeated motion.
2. Sucking blister on baby lip: is it normal?
Yes, in many newborns, it is normal.
A baby’s lips do a surprising amount of work during feeding. The orbicularis oris muscle strain involved in creating and maintaining suction can contribute to local rubbing on the lip surface. In our editorial review of pediatric and lactation guidance, this is one reason lip blisters are commonly seen in otherwise healthy babies.
A normal sucking blister usually has these features:
- Located on the upper lip, often near the center
- Small and localized
- Clear, pale, or slightly thickened
- Appears during periods of frequent feeding
- Does not cause fever or widespread mouth sores
A brief real-world example: a 6-day-old infant in a feeding clinic developed a small central upper-lip blister after cluster feeding. The baby fed well, gained weight, and had no white patches inside the cheeks or tongue. The blister faded on its own over the following days after latch adjustments.
That pattern is typical.
3. What causes a sucking blister?
Several feeding-related factors can contribute. The blister itself is usually caused by friction, but the reason for excess friction may vary.
Common clinical causes
A strong sucking reflex
Newborns are wired to suck. That reflex helps with feeding and self-soothing. Some infants suck so vigorously that the lip skin repeatedly rubs against the breast, bottle nipple, or even their own hands.
Shallow latch during breastfeeding
The phrase suck blister baby lip shallow latch comes up often in parent searches for a reason. A shallow latch can increase pressure on the lip instead of distributing it more evenly through the mouth and areola. That repeated rubbing may trigger blister formation.
Bottle feeding mechanics
A newborn lip blister from bottle feeding may happen if:
- The nipple flow is too slow, causing harder sucking
- The nipple shape does not match the baby’s oral mechanics
- Feeding sessions are prolonged
- The bottle angle affects suction and lip tension
Lip tie or oral restriction
Sometimes a lip tie or tongue movement issue changes how the baby seals around the nipple. This can increase friction. Not every lip blister means there is an oral tie, but persistent feeding difficulty may justify assessment by a pediatrician or IBCLC.
Sensitive skin
Some newborns simply have more delicate skin. Their lips may blister more easily even when feeding is otherwise going well.
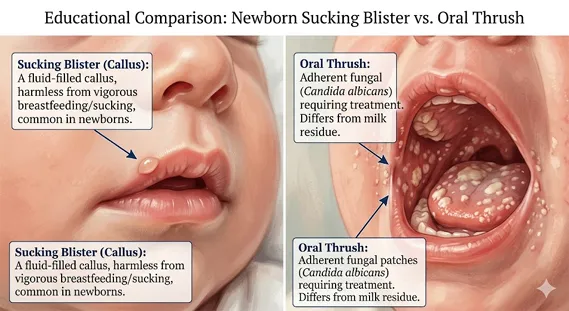
4. Sucking blister vs thrush: how can parents tell the difference?
This is one of the most important questions. The sucking blister vs thrush distinction matters because the two conditions look different and are managed differently.
Thrush is a yeast infection. A sucking blister is a friction lesion.
Quick comparison table
| Feature | Sucking Blister | Oral Thrush |
|---|---|---|
| Usual location | Upper lip, localized spot | Tongue, inner cheeks, gums, sometimes lips |
| Appearance | Clear, yellowish, or callused blister | White creamy patches that may look like milk residue |
| Cause | Friction from sucking | Candida yeast overgrowth |
| Pain | Often minimal or none | May cause soreness or fussiness |
| Feeding impact | Usually mild or none | May lead to feeding discomfort |
| Contagious? | No | Yeast can affect both baby and breastfeeding parent |
| Treatment | Usually none; improve latch/feeding mechanics | Medical evaluation and antifungal treatment may be needed |
An oral thrush infant comparison also helps clarify another point: milk residue wipes away easily, but thrush patches often do not. Thrush may also involve diaper rash or nipple pain in the breastfeeding parent.
For trusted guidance, see the NHS oral thrush in babies resource.
5. Hidden causes: shallow latch, lip ties, and friction
Not every blister means there is a feeding problem. But when we review patient histories, recurring blisters often overlap with latch concerns.
Signs a shallow latch may be contributing
- Clicking sounds during feeding
- Lip curling inward rather than flanging outward
- Frequent unlatching
- Nipple pain during breastfeeding
- Poor milk transfer
- Long, tiring feeds
A baby with a shallow latch may use the lips to compensate for less effective suction deeper in the mouth. That can create a friction point on the upper lip.
What about lip ties?
Lip ties are controversial in some settings because not every visible frenulum causes symptoms. Still, if a baby has:
- Ongoing latch difficulty
- Poor weight gain
- Persistent maternal nipple pain
- Recurrent lip blistering
- Trouble maintaining suction
then a functional feeding assessment may be more useful than looking at the lip alone.
For many families, the best next step is not guessing online. It is skilled observation during a feed.

6. How to treat infant friction blisters safely
Parents frequently ask how to treat infant friction blisters. The answer is usually simple: do less, not more.
In most cases, treatment focuses on protecting the area and correcting the source of friction.
What usually helps
- Continue feeding if baby is comfortable
- Improve latch and positioning
- Check bottle nipple size and flow
- Let the blister heal naturally
- Monitor for changes
What to avoid
- Do not pop the blister
- Do not peel the skin
- Do not apply adult oral gels unless a clinician recommends them
- Avoid herbal or home remedies that may irritate newborn skin
Some parents use a small amount of expressed breast milk on the lip. While evidence is limited, it is commonly used in infant care and may be soothing. The main priority, however, is reducing friction.
If you are breastfeeding, support from an International Board Certified Lactation Consultant may help refine positioning and seal. For broader infant feeding recommendations, the American Academy of Pediatrics breastfeeding guidance is also useful.
7. Bottle feeding and sucking blisters: does it happen?
Yes. A newborn lip blister from bottle feeding is absolutely possible.
Bottle-fed babies can develop the same kind of friction lesion, especially if they:
- Work hard to draw milk
- Use a nipple with an awkward shape
- Feed for long periods
- Clamp with the lips to stabilize the nipple
Parents sometimes assume a lip blister only happens in breastfed infants. That is not the case. What matters most is the mechanics of suction and friction.
Bottle-feeding tips that may help
- Use an age-appropriate nipple flow
- Watch for lip curling or dimpling
- Try paced bottle feeding
- Keep feeds calm and upright
- Replace worn nipples regularly
This matters because a baby who overworks the lips may also swallow extra air, leading parents to wonder about related concerns like reflux, gas, or even sleep-position questions such as When should you start using a baby pillow. For safety, though, pillows are not recommended for newborn sleep.
8. When should you see a pediatrician or lactation consultant?
A sucking blister is usually harmless. But there are times when it makes sense to get expert help.
Contact a clinician if:
- The blister is large, bleeding, or rapidly worsening
- Your baby seems in pain during feeds
- There are white patches inside the mouth
- Your baby has fever or appears unwell
- Feeding is ineffective or weight gain is poor
- You suspect dehydration
- The lesion does not improve or keeps returning
See a lactation consultant if:
- Breastfeeding is painful
- Your baby has a persistent shallow latch
- Feeds are very long or very frequent without satisfaction
- You hear clicking
- You suspect oral restriction
In clinical practice, the blister itself is rarely the true problem. It is often the clue.
9. Are sucking blisters ever dangerous?
Usually, no. They fall into the broad group of benign newborn skin lesions. They do not generally cause long-term oral damage, dental issues, or developmental harm.
Still, the differential diagnosis matters. A lesion that looks unusual could occasionally reflect something else, such as:
- Oral thrush
- Herpes infection
- Traumatic injury
- Rare skin conditions
That is why location, appearance, and the baby’s overall health matter more than the blister alone.
Most consensus-based guidance from pediatric and public health sources supports a conservative approach when the baby is feeding well and has no other symptoms.
10. Prevention strategies that actually help
You cannot always prevent a sucking blister. Some babies develop one despite excellent feeding support. But you can often reduce the risk.
Breastfeeding prevention tips
- Aim for a deep latch
- Bring baby to breast, not breast to baby
- Check that lips are flanged outward
- Reposition if feeding is painful
- Ask for help early with breastfeeding latch technique
Bottle-feeding prevention tips
- Choose the correct nipple flow
- Avoid forcing longer feeds
- Try paced feeding
- Watch your baby’s mouth seal and lip position
Parent education matters
One of the most helpful interventions is reassurance. New parents are often exhausted and alert to every small change. A tiny lip blister can trigger major anxiety, especially if they are also watching stools, spit-up, and weight. That is why topics like Undigested Milk in Baby Stool or Blood in Baby Stool often appear in the same stretch of newborn care concerns.
Frequently Asked Questions
1. Do sucking blisters hurt babies?
Usually not much. Most babies continue feeding normally. If your baby seems distressed or refuses feeds, a pediatric assessment is wise.
2. How long does a sucking blister last?
Many resolve within days to a couple of weeks. If friction continues, the blister may persist or recur.
3. Can breastfeeding cause a sucking blister?
Yes. Breastfeeding can be associated with a sucking blister, especially if there is a shallow latch. That does not mean breastfeeding should stop. It often means latch support may help.
4. How do I know if it is sucking blister vs thrush?
A sucking blister is usually a single localized lip lesion. Thrush tends to cause white patches inside the cheeks, tongue, or gums. If you’re unsure, your pediatrician can help distinguish sucking blister vs thrush.
5. Should I put cream or medicine on it?
Usually no. For how to treat infant friction blisters, the safest approach is often observation and feeding adjustment. Avoid medicated products unless your clinician recommends them.
6. Can bottle feeding cause it too?
Yes. A newborn lip blister from bottle feeding can happen if nipple flow, shape, or feeding mechanics increase friction.
Conclusion
A sucking blister in a newborn is usually a small, harmless sign of friction from feeding rather than a dangerous condition. It may appear with breastfeeding, finger sucking, or bottle feeding. The key is to look at the full picture: how the lesion looks, whether your baby is feeding well, and whether there are signs of infection or latch problems.
In our clinical review, the most helpful approach is simple. Observe closely. Support effective feeding. Get help if the blister is persistent, painful, or paired with poor weight gain, white mouth patches, or other symptoms. For many families, a calm explanation and a few feeding adjustments are all that is needed.
If you are tracking other newborn health questions alongside feeding issues, it may also help to review Undigested Milk in Baby Stool, Blood in Baby Stool, and When should you start using a baby pillow as part of a broader, safety-focused care plan.
References
- NHS. oral thrush in babies
- International Board of Lactation Consultant Examiners. International Board Certified Lactation Consultant
- American Academy of Pediatrics. American Academy of Pediatrics breastfeeding guidance
Usually not much. Most babies continue feeding normally. If your baby seems distressed or refuses feeds, a pediatric assessment is wise.
Many resolve within days to a couple of weeks. If friction continues, the blister may persist or recur.