


Job Title: Orthopaedic Surgeon
Institutional Affiliation: Royal Brisbane and Women’s Hospital (Queensland, Australia)
Specialties: Musculoskeletal Health | Orthopaedic Surgery | Long-Term Mobility Care
Dr. John Ma is a dedicated Orthopaedic Surgeon with extensive experience in musculoskeletal health and advanced surgical care. At Healthy Post, Dr. Ma directly authors and writes comprehensive musculoskeletal health guides, combining contemporary evidence‑based clinical practice with compassionate care to help individuals achieve long-term wellness.
Verify Medical Credentials:

Medically Reviewed By
Dr. Himanshu Gupta, MS (Ortho)
Orthopedic & Robotic Joint Replacement Specialist
Dr. Himanshu Gupta is a distinguished Orthopedic Surgeon and the Chief Director at Amicare Hospital with over 20 years of clinical experience. He specializes in robotic-assisted joint replacement, arthroscopy, and complex sports injury rehabilitation. Dr. Gupta is dedicated to ensuring the highest standards of medical accuracy and evidence-based care in all orthopedic content he reviews.
Orthopedic Surgery Review & Editorial Verification
This comprehensive clinical guide on the diagnosis, conservative therapy, and surgical intervention pathways for radial tunnel syndrome was written by Dr. John Ma, Specialist in Orthopedic Surgery. All diagnostic criteria, comparative matrices, and rehabilitation insights have been fact-checked and clinically verified to conform strictly to global musculoskeletal and upper extremity orthopedic standards.
Medical Disclaimer: The clinical guidelines and therapeutic protocols outlined in this article are intended solely for educational awareness and patient advocacy. Radial nerve entrapment pathologies share highly overlapping clinical signs with common tendonitis variants. This information does not substitute for a formal clinical evaluation or nerve conduction study. Always consult a qualified orthopedic specialist, hand surgeon, or physical therapist if you experience persistent outer elbow pain, forearm fatigue, or loss of extremity function.
A nagging ache on the outside of the elbow can be surprisingly hard to name. In clinic notes and patient histories, we often see radial tunnel syndrome mistaken for tennis elbow, delayed for months, or dismissed as “just overuse.” That matters. When the wrong diagnosis sticks, people may keep lifting, typing, gripping, or training through pain that needs a different plan. If your forearm pain feels deep, stubborn, and worse with rotation or extension, this condition deserves a closer look.
It is also a reminder that not every elbow problem starts in the tendon. Sometimes the issue involves a nerve. In this case, the posterior interosseous nerve, a radial nerve branch, becomes irritated as it passes through a tight space in the upper forearm called the radial tunnel. The result is usually pain, not paralysis. And in 2026, most expert guidance still favors conservative care first: activity changes, medication when appropriate, splinting, and structured rehabilitation.
Patients dealing with upper-limb pain often have broader musculoskeletal questions too. On orthopedic education sites, they may also search for Why Does My Knee Click But No Pain, How to Sleep After Hip Replacement, or Orthopedic Bone Screws while trying to understand how healing, biomechanics, and nerve irritation overlap.
1. What is radial tunnel syndrome?
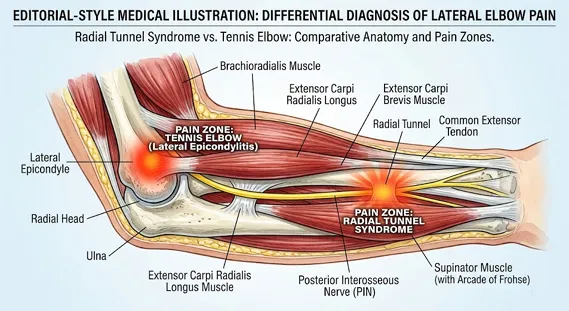
Radial tunnel syndrome is a compression-related pain condition involving the posterior interosseous nerve as it travels through the proximal forearm. The radial tunnel is not a single point. It is a pathway bordered by muscles, fascia, and fibrous structures near the elbow. One common pressure point is the arcade of Frohse, part of the supinator muscle.
This condition is considered uncommon, with estimates around 3 cases per 100,000 people per year. It appears most often in adults between 30 and 50. Women may be affected slightly more often than men, though the data are limited.
Why it is missed:
- The pain can mimic lateral epicondylitis, better known as tennis elbow
- MRI findings are often normal
- A nerve conduction study may not clearly confirm it
- There is ongoing debate about whether some cases overlap with other forearm pain syndromes
That is why many experts describe it as a diagnosis of exclusion. In plain language, clinicians often arrive at it after ruling out more common causes of elbow and forearm pain.
2. Radial tunnel syndrome symptoms: what patients usually notice
The most recognizable radial tunnel syndrome symptoms are pain-based rather than numbness-based. Unlike classic nerve injuries that cause tingling or weakness, this syndrome usually creates a deep, aching discomfort.
Common symptoms include:
- Deep ache in the dorsoradial forearm
- Pain about 3 to 5 cm below the lateral epicondyle
- Worsening pain with forearm rotation
- Pain with wrist extension or lifting
- Tenderness over the radial tunnel
- Night pain or a heavy, fatigued feeling in the forearm
A practical example: a patient may say, “It hurts when I turn a screwdriver, pour from a heavy pan, or hold my wrist up while typing.” That pattern can be a clue.
One important distinction: radial tunnel syndrome usually does not cause true sensory loss or muscle paralysis. If a person cannot extend the fingers or wrist because of actual motor failure, clinicians must think about posterior interosseous nerve palsy or another neurologic condition.
3. Radial tunnel syndrome vs tennis elbow: why the difference matters
The phrase radial tunnel syndrome vs tennis elbow comes up so often because the two conditions can look similar at first glance. Both may cause outer elbow pain. Both may worsen with hand use. But the pain location and exam findings are not the same.
| Feature | Radial Tunnel Syndrome | Tennis Elbow |
|---|---|---|
| Main pain site | 3–5 cm distal to lateral epicondyle | Directly over lateral epicondyle |
| Pain quality | Deep, nagging ache | Sharp pain with gripping or lifting |
| Aggravating motions | Supination, wrist extension, forearm rotation | Gripping, wrist extension, lifting |
| Nerve findings | Usually no numbness or paralysis | No nerve compression pattern |
| Exam clue | Pain with resisted supination or resisted middle finger extension | Point tenderness at lateral epicondyle |
| Coexistence | May coexist in a small number of cases | Often the primary diagnosis |
In real practice, overlap can happen. A patient may have tendon pain and nerve irritation at the same time. That is one reason outcomes may be slower when the picture is mixed.
For readers exploring related orthopedic pain patterns, this confusion is not unlike the way people compare joint sounds and symptoms in Why Does My Knee Click But No Pain—location, triggers, and function all matter.
4. How doctors diagnose radial tunnel syndrome in 2026
There is no single perfect test. Diagnosis depends on the story, the exam, and ruling out other causes.
Key clinical tests
A careful musculoskeletal and neurologic exam remains central. Common maneuvers include:
- Resisted middle finger extension test: pain reproduced over the radial tunnel
- Resisted supination test: pain when turning the forearm outward against resistance
- Rule of Nine test: a pressure grid used to localize tenderness in the proximal forearm
These tests are not flawless, but together they help build a pattern.
Imaging and electrodiagnostics
MRI may be ordered to exclude other problems or to look for muscle edema or denervation changes. Still, many patients with convincing symptoms have normal scans.
A nerve conduction study or EMG is often done when clinicians need to rule out cervical radiculopathy, PIN palsy, or more diffuse nerve disease. In radial tunnel syndrome, electrodiagnostic findings are frequently normal or inconclusive. That does not rule the condition out, but it does limit test certainty.
Conditions that may mimic it
Doctors often consider:
- Lateral epicondylitis
- Posterior interosseous nerve palsy
- Cervical nerve root irritation
- Elbow arthritis
- Synovial or ganglion masses
- Referred pain from shoulder or neck dysfunction
Most studies agree on one point: radial tunnel syndrome remains a clinical diagnosis supported by exclusion rather than a lab-confirmed disease.
For evidence-based overviews, clinicians often refer to NHS guidance for general nerve and musculoskeletal care, NICE recommendations on assessment pathways, and peer-reviewed summaries indexed in PubMed.
5. First-line treatment: what current guidelines favor
The 2025–2026 consensus is clear. Initial care should be conservative unless there is another urgent diagnosis.
Activity modification and rest
This is not the same as complete inactivity. It usually means reducing repetitive:
- Pronation and supination
- Forceful gripping
- Repeated wrist extension
- Tool use, racquet sports, or heavy lifting that reproduces symptoms
In our editorial review of rehabilitation plans, patients tend to do better when they understand why a movement irritates the tunnel. That insight makes compliance easier.
Medications and injections
Nonsteroidal anti-inflammatory drugs may help reduce pain in some patients, especially during flare-ups. A corticosteroid injection may also be considered in select cases, though techniques and outcomes vary. It can reduce local inflammation, but it is not a guaranteed fix.
Splinting
Wrist splinting or elbow support is often used, especially at night or during aggravating tasks. The goal is to reduce strain on the extensor-supinator region and calm symptoms enough for therapy to begin.
6. Radial tunnel syndrome physical therapy: the 2026 rehabilitation shift
Among all nonoperative options, radial tunnel syndrome physical therapy remains one of the most important. The newer rehabilitation trend is not aggressive strengthening on day one. It is staged, symptom-guided progression.
A skilled therapist may include:
- Gentle extensor and supinator stretching
- Nerve gliding for the radial nerve pathway
- Soft tissue mobilization to reduce tissue restriction
- Scapular and shoulder mechanics work
- Gradual grip and forearm strengthening
- Closed-chain loading when tolerated
- Proprioceptive retraining
This matters because elbow pain is often a chain problem, not just a local one. If the shoulder, wrist, and posture are poorly coordinated, the forearm absorbs more strain.
Radial tunnel syndrome exercises patients may be taught
The best radial tunnel syndrome exercises depend on pain level and stage of recovery, but common examples include:
- Radial nerve glides
- Gentle wrist extensor stretches
- Isometric wrist extension
- Forearm supination/pronation control with light resistance
- Progressive grip strengthening once pain settles
These should be taught with caution. If an exercise reproduces sharp or lasting pain, it may need adjustment. More is not always better.
A short clinical example: one office worker improved after changing keyboard height, using a nighttime splint, and starting nerve glides plus shoulder stabilization. Another patient with persistent symptoms needed a longer program because tennis elbow was also present. Same diagnosis family. Different recovery curve.

7. When surgery is considered
Surgery is generally reserved for patients who do not improve after a substantial trial of conservative treatment. Exact timing varies, but many specialists consider surgery only after several months of persistent symptoms and a careful re-evaluation of the diagnosis.
The procedure is usually called radial tunnel release. It involves decompressing structures that may be irritating the nerve, including the arcade of Frohse and tight fascial bands around the supinator.
What patients should know about outcomes
Reported success rates often range from 70% to 90%, but those numbers need context.
- Recovery may take 9 to 18 months
- Improvement may be gradual rather than immediate
- Outcomes can be less predictable if tennis elbow coexists
- Multiple entrapment neuropathies may reduce success
That is one reason many modern treatment pathways emphasize rehabilitation before surgery. Functional recovery matters more than a quick operation if symptoms can be controlled without it.
8. 2026 treatment guidelines: what is new?
The core principles have not changed dramatically, but the emphasis has.
Current consensus points
- Radial tunnel syndrome is still a diagnosis of exclusion
- Conservative care remains first-line treatment
- Rehabilitation is more structured and progressive than in older protocols
- Early surgery is generally not favored without strong reasons
- Coexisting tendon or cervical issues should be addressed, not ignored
What has shifted in practice
Recent reviews highlight:
- Better use of nerve gliding within graded rehab
- More focus on kinetic-chain deficits
- Wider use of patient-specific return-to-work modifications
- Less reliance on imaging alone
- Greater caution when interpreting inconclusive electrodiagnostic tests
This aligns with broader orthopedic trends seen across upper-limb recovery, implants, and post-op care topics such as Orthopedic Bone Screws and How to Sleep After Hip Replacement. Modern musculoskeletal care is increasingly function-focused, not just anatomy-focused.
9. Practical self-care tips patients can use now
If you suspect radial tunnel irritation, these steps may help while you wait for assessment:
- Reduce repetitive twisting and lifting
- Avoid prolonged gripping with the wrist extended
- Consider temporary wrist splinting at night
- Use ergonomics to lower forearm strain at work
- Track which motions trigger pain
- Start only clinician-approved radial tunnel syndrome exercises
Seek medical care sooner if you develop:
- True hand or finger weakness
- Loss of finger extension
- Numbness that spreads or worsens
- Severe swelling, trauma, or neck-related neurologic symptoms
FAQs
Is radial tunnel syndrome serious?
It is usually not dangerous, but it can become chronic and disruptive if missed. Persistent pain can affect work, sleep, exercise, and daily tasks.
How is radial tunnel syndrome different from posterior interosseous nerve palsy?
Radial tunnel syndrome mainly causes pain. Posterior interosseous nerve palsy causes motor weakness, such as difficulty extending the fingers or thumb.
Do radial tunnel syndrome exercises really help?
They may help when chosen carefully and progressed gradually. The best results usually come from guided rehabilitation rather than random online routines.
Can a nerve conduction study confirm radial tunnel syndrome?
Not reliably in many cases. A nerve conduction study is often more helpful for ruling out other nerve disorders than proving this one.
Is a corticosteroid injection always necessary?
No. A corticosteroid injection may be considered in selected patients, but many improve with rest, splinting, and radial tunnel syndrome physical therapy.
Can radial tunnel syndrome happen along with tennis elbow?
Yes. That overlap is one reason the radial tunnel syndrome vs tennis elbow discussion is so important in diagnosis and treatment planning.
Conclusion
Radial tunnel syndrome is uncommon, but the pain is real, and the diagnostic confusion is common. The key clues are location, movement triggers, and the absence of classic numbness or paralysis. In 2026, the strongest consensus still supports conservative treatment first: activity modification, medication when appropriate, splinting, and well-designed radial tunnel syndrome physical therapy. Surgery remains an option for resistant cases, but only after careful reassessment.
If forearm pain has lingered for weeks, especially if it worsens with rotation or resisted middle finger extension, it is worth discussing with a qualified clinician. Early recognition may reduce prolonged pain, prevent unnecessary procedures, and get you back to work, sport, and sleep with a clearer plan. Patients researching related orthopedic concerns may also find value in Why Does My Knee Click But No Pain, How to Sleep After Hip Replacement, and Orthopedic Bone Screws as part of a broader recovery education journey.