

Living with type 2 diabetes can feel overwhelming at times 😔. Doses, blood sugar numbers, and side effects all add up. If your doctor has prescribed glimepiride, you might be wondering whether 2mg or 4mg is safer or more effective for you.
This guide breaks down the differences between glimepiride 2mg and glimepiride 4 mg in clear, practical language. You will learn what the medicine is used for, how it works, and how to use it more safely with your healthcare team.
Fact 1: What glimepiride 2mg and 4 mg are really used for
First, let’s answer a basic question many people ask: What is glimepiride used for?
Glimepiride (DrugBank ID: DB00222) is a prescription tablet for type 2 diabetes mellitus (T2DM). It belongs to a group of medicines called sulfonylureas. It was first approved by the U.S. FDA in 1995 and is sometimes called a second- or third-generation sulfonylurea.
You may see it sold under brand names like:
- Amaryl
- Duetact (glimepiride + pioglitazone)
- Tandemact (glimepiride + pioglitazone in some regions)
Main purpose in everyday care
This medicine is:
- An add-on to diet and exercise for adults with type 2 diabetes.
- Used as monotherapy (alone) or in combination therapy with:
- Metformin
- Insulin
- Pioglitazone
- Rosiglitazone
In clinical studies, this sulfonylurea typically:
- Lowers fasting plasma glucose by about 46 mg/dL
- Lowers post-meal glucose by about 72 mg/dL
- Reduces HbA1c by about 1.4%
That kind of drop can make a real difference in diabetes control and long-term complications 👍.
Where do 2mg and 4mg fit?
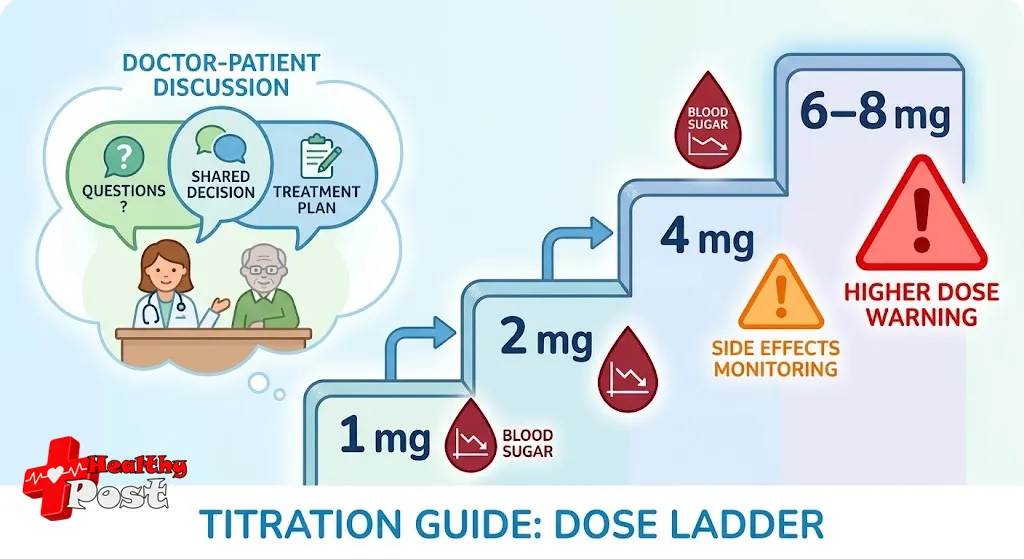
Most people start at a low dose and slowly go up:
- A common starting dose is 1–2 mg once daily.
- The dose may rise by 1–2 mg at a time.
- Many people end up on 2–4 mg once daily.
- Some may need up to 8 mg daily, depending on response and safety.
So:
- glimepiride 2mg is often used as a starting or early step-up dose.
- glimepiride 4 mg is usually for people who need stronger glucose lowering after trying lower doses.
Both doses have the same purpose: helping your pancreas release more insulin to control blood sugar. The key difference is how strong the effect is and how high your risk of low sugar becomes.

Fact 2: How this diabetes medicine works inside your body
To use this drug safely, it helps to know how it lowers blood sugar.
Step-by-step mechanism of action
This sulfonylurea mainly targets ATP-sensitive potassium (KATP) channels on pancreatic beta cells:
- It blocks KATP channels on beta cells.
- The cell membrane depolarizes (its electrical charge changes).
- This opens voltage-dependent calcium channels, allowing calcium to enter the cell.
- The calcium influx triggers exocytosis of insulin granules.
- More insulin enters the bloodstream, which lowers blood sugar.
In addition, it:
- May improve how sensitive muscles and fat are to insulin.
- Helps peripheral tissues take up more glucose from the blood.
Pharmacology: how the body handles the drug
Understanding how the medicine moves through your body can also explain why timing and dosing matter.
Absorption and onset
- Rapidly and almost completely absorbed after swallowing.
- Reaches peak blood levels in 2–3 hours.
- Absorption starts within the first hour.
- Has nearly complete bioavailability (most of the dose reaches circulation).
Distribution and binding
- Very high protein binding: more than 99.5% attaches to plasma proteins.
- This means it can be affected by other drugs that compete for protein binding.
Metabolism and elimination
- Primarily broken down in the liver by CYP2C9.
- First creates an active metabolite (M1).
- Then forms an inactive metabolite (M2).
- Around 60% is excreted in urine, mostly as metabolites.
- Around 40% is excreted in feces, also mainly as metabolites.
Half-life and duration
- Has a half-life of about 5–8 hours.
- With repeated dosing, it can extend up to 9 hours.
- Clearance is around 48–52 mL/min.
This relatively long duration of action is why:
- It is often taken once daily, usually with breakfast or the first main meal.
- Both 2mg and 4mg doses can keep working through the day.
- The risk of low sugar can sometimes extend into the evening or night.
Fact 3: Dose differences, timing, and who should start where
Many people worry they are on “too strong” a dose. The real question is whether the dose is matching your body’s needs.
2mg vs 4mg: what changes?
In general:
- 2mg
- Often a starting dose for adults.
- Used in people who are older, lean, have kidney or liver issues, or are sensitive to lows.
- Provides a gentler boost in insulin.
- 4mg
- A step-up dose when lower doses do not control blood sugar enough.
- May be chosen for younger or heavier patients, or those with high baseline glucose.
- Brings a stronger glucose-lowering effect, but with higher hypoglycemia risk.
Typical dose-titration strategy
Your healthcare professional may follow a pattern like this:
- Start low
- 1–2 mg once daily with breakfast.
- Check response after about 1–2 weeks
- Review fasting and post-meal blood sugars.
- Consider HbA1c at about 3 months.
- Increase gradually
- Raise by 1–2 mg at a time, not more often than weekly.
- Move from 2 mg → 3–4 mg only if needed.
- Avoid going too high
- Many guidelines keep daily doses at or below 8 mg.
- Higher doses rarely add benefit but raise the risk of lows.
The choice between 2mg and 4mg is not about “strong vs weak” people. It is about balancing glucose control and safety.
Timing with meals
Because the drug boosts insulin release, it usually works best when:
- Taken once daily with the first substantial meal.
- Some people split doses (for example, 4mg as 2mg twice daily) if advised.
Important points:
- Never skip meals after taking it.
- If you eat much less than usual, your risk of low sugar increases.
- Alcohol, fasting, or intense exercise can raise that risk even more.
Special groups: who needs extra caution?
You should discuss lower starting doses (often 1mg or 2mg) if you:
- Are age 65 or older.
- Have reduced kidney function.
- Have liver disease.
- Have a history of frequent hypoglycemia.
- Take other medicines that lower glucose (like insulin or other secretagogues).
For some people, especially with advanced kidney disease or very unpredictable eating patterns, other medicines may be safer than any sulfonylurea.
Fact 4: Safety, hypoglycemia, and other glimepiride side effects
No diabetes medicine is risk-free. Being informed helps you respond early and stay safer 💙.
Hypoglycemia: the main concern
Compared with older sulfonylureas like glyburide, this drug has a lower risk of hypoglycemia. However, serious lows can still happen, especially at higher doses such as 4mg or more.
Risk is higher if you:
- Take too high a dose for your needs.
- Skip or delay meals after taking your tablet.
- Exercise more than usual without adjusting food intake.
- Drink alcohol, especially on an empty stomach.
- Have kidney or liver problems.
- Use it together with insulin or other glucose-lowering drugs.
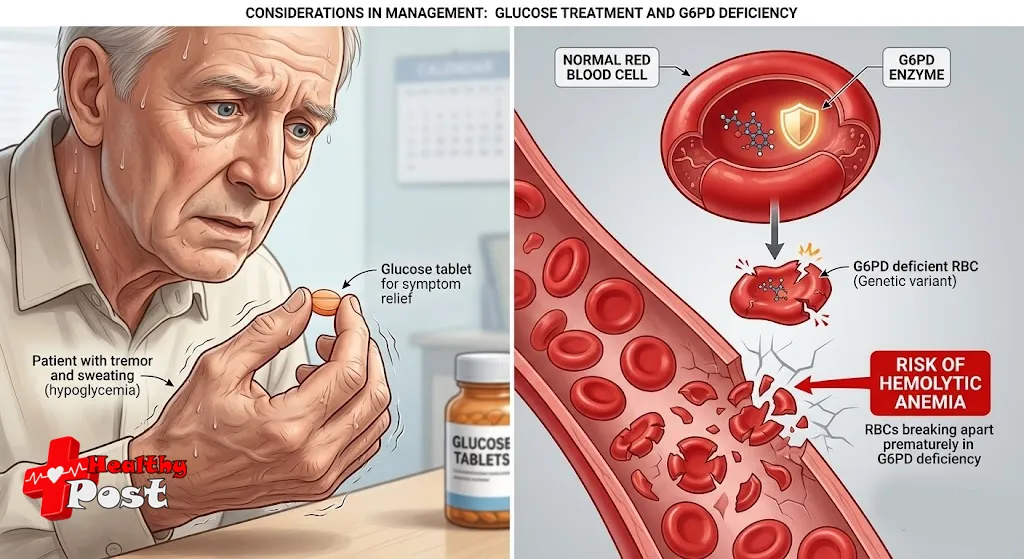
Common low-sugar symptoms include:
- Shakiness or tremor
- Sweating, chills
- Fast heart rate
- Sudden hunger
- Blurred vision
- Irritability, confusion, or headache
Severe hypoglycemia can cause:
- Seizures
- Loss of consciousness
- Rarely, coma
That is why glimepiride side effects always need to be taken seriously.
What to do if you suspect a low
If you are awake and able to swallow safely:
- Check your blood glucose if possible.
- If it is below about 70 mg/dL, or if you strongly suspect a low:
- Take 15–20 grams of fast-acting carbohydrate:
- 4 glucose tablets, or
- 1/2 cup regular soda or juice, or
- 1 tablespoon sugar or honey.
- Take 15–20 grams of fast-acting carbohydrate:
- Recheck in 15 minutes.
- Repeat if still low.
- Eat a snack or meal once your sugar rises, to keep it stable.
If the person is unconscious or cannot swallow, call emergency services immediately 🚑.
Other side effects to know
Besides low blood sugar, other possible side effects include:
- Weight gain
- Usually less pronounced than with some older sulfonylureas.
- Still possible, especially at higher doses or with extra snacking.
- Digestive issues
- Nausea
- Stomach discomfort
- Rarely, diarrhea or constipation
- Allergic reactions (uncommon)
- Rash
- Itching
- Hives
- Very rare severe reactions may involve breathing problems or swelling.
- Blood cell effects (rare)
- Very low white blood cells or platelets.
- Signs may include unusual bruising, infections, or fatigue.
- Liver enzyme changes
- Rare cases of elevated liver tests have been reported.
- Unexplained fatigue, yellowing of skin or eyes, or dark urine need attention.
Long-term safety, toxicity, and cancer data
From animal studies and safety reviews:
- Oral LD50 in rats is greater than 10,000 mg/kg, indicating low acute toxicity.
- In rats, no evidence of carcinogenicity was found.
- In mice given very high doses, benign pancreatic adenomas were observed.
- Standard tests showed no mutagenic effects.
- Fertility in rats was not affected.
These data are reassuring, but they do not replace long-term human vigilance. Regular medical follow-up remains important.
Pharmacogenomics: G6PD deficiency and hemolytic anemia
Some people carry genetic variants in the glucose-6-phosphate dehydrogenase (G6PD) gene. In these patients, certain medicines can trigger hemolytic anemia (destruction of red blood cells).
For this drug:
- G6PD deficiency is considered a risk factor.
- Affected patients may develop:
- Fatigue
- Pale skin
- Shortness of breath
- Dark urine
- Yellowing of the eyes
If you know you have G6PD deficiency, tell your clinician and pharmacist. You may still use this medicine in some cases, but:
- You should be monitored closely.
- Your team may choose alternative drugs if risk seems high.
Fact 5: How this drug compares with other sulfonylureas
People often ask whether they should be on this medicine at all, or switch to another sulfonylurea like glipizide or glyburide.
Comparison with two common sulfonylureas
Here is a simplified comparison:
| Feature | This medicine (e.g., Amaryl) | Glipizide | Glyburide |
|---|---|---|---|
| FDA approval year | 1995 | 1984 | 1984 |
| Generation | Second / third | Second | Second |
| Duration of action | Longer | Shorter | Moderate |
| Dosing frequency | Often once daily | Often twice daily | Once or twice daily |
| Hypoglycemia risk | Lower | Moderate | Higher |
| Weight gain | Lower | Moderate | Higher |
| Heart (cardiac) effects | Minimal impact | Moderate impact | More significant impact |
| Common use with metformin | Yes | Yes | Less favored in some cases |
Key takeaway:
- This agent offers strong glucose-lowering with:
- Less weight gain
- Lower hypoglycemia risk
- Less disruption of ischemic preconditioning in heart tissue
This is one reason many clinicians prefer it over glyburide, especially in older adults or those with heart disease.
Clinical scenarios for 2mg vs 4mg within this class
Imagine two brief examples (for illustration only):
- Maria, 68 years old
- Slim, mild kidney impairment, lives alone.
- Doctor chooses glimepiride 2mg once daily, with slow titration.
- Goal: reasonable glucose control with minimal risk of severe lows.
- David, 52 years old
- Overweight, high baseline HbA1c, works regular hours.
- After trying 2mg, his sugars remain high.
- Doctor increases to glimepiride 4 mg, with close monitoring.
- Goal: stronger insulin stimulation, but with robust education on hypoglycemia.
These examples show how individual factors, not just the number on the pill, guide safe choices.
Practical tips for safer daily use of 2mg and 4mg doses
No matter which dose you take, a few habits can dramatically improve safety and effectiveness.
1. Build a routine around meals
- Take your tablet with breakfast or your first main meal.
- Try to eat at similar times each day.
- Keep a small source of fast sugar with you, such as glucose tablets.
2. Track your numbers
- Check fasting blood sugars at least as recommended.
- If you can, check post-meal readings when doses change.
- Bring your log or meter to appointments 📊.
3. Watch for patterns, not single readings
- One low or one high does not always require a dose change.
- Repeated morning lows may mean your dose is too high.
- Persistently high fasting or post-meal sugars may suggest a need to adjust dose or add another drug.
4. Know when to call your healthcare team
Reach out promptly if:
- You have repeated hypoglycemia, especially at night.
- Your blood sugar often exceeds 250–300 mg/dL despite taking it correctly.
- You experience new chest pain, shortness of breath, or severe fatigue.
- You notice signs of allergic reaction or unusual bruising.
5. Remember: this article is not personal medical advice
This information is meant to support, not replace, conversations with your clinician. Your situation may involve:
- Other chronic conditions
- Different medications
- Pregnancy or plans for pregnancy
- Kidney or liver function issues
These factors all influence whether 2mg, 4mg, or another treatment entirely is best for you.

FAQs about glimepiride 2mg vs 4mg
1. Is 4mg twice as strong as 2mg?
Not exactly, but 4mg generally has a stronger effect on insulin release than 2mg. The relationship is not perfectly linear. Your response depends on:
- Pancreatic function
- Body size
- Other medications
- Kidney and liver health
2. Can I switch from 4mg back to 2mg if I have lows?
Often, yes, doses can be reduced. However, never change your dose on your own. Call your healthcare professional first. They may:
- Lower the dose
- Adjust other medicines
- Change meal plans
- Consider a different drug class
3. Can I split a 4mg tablet to make 2mg?
If your tablet is scored and your pharmacist agrees, some 4mg tablets can be split in half. However:
- Not all formulations are suitable for splitting.
- Always check the exact brand and tablet design.
- Ask your pharmacist before cutting any tablet.
4. Is this medicine safe with metformin?
Yes, it is commonly combined with metformin. The two drugs work in different ways:
- Metformin reduces glucose production in the liver and improves insulin sensitivity.
- This sulfonylurea stimulates insulin release from the pancreas.
Together, they often provide stronger HbA1c reduction than either alone. But the combination may increase hypoglycemia risk, especially at higher sulfonylurea doses.
5. Does this drug cause weight gain?
It can cause some weight gain, though usually less than with older sulfonylureas like glyburide. Reasons include:
- More insulin available
- More glucose stored in tissues
- Extra calories from treating low sugars
Balanced nutrition and regular movement can help limit this effect.
6. Is it safe for people with heart disease?
Compared with some other sulfonylureas, this one seems to have minimal effect on ischemic preconditioning (a protective heart mechanism). That is considered an advantage. Still:
- People with heart disease require careful overall diabetes management.
- Your cardiologist and diabetes specialist should coordinate your care.
Conclusion: Using glimepiride thoughtfully for safer diabetes control
Choosing between glimepiride 2mg and glimepiride 4 mg is about much more than the number printed on the tablet. It is about your blood sugar patterns, age, other illnesses, medications, and how likely you are to experience hypoglycemia.
Key points to remember:
- This sulfonylurea was approved in 1995 and remains a reliable option for type 2 diabetes.
- It works by stimulating insulin release and slightly improving insulin sensitivity.
- Dosing should start low and go slow, especially in older adults or those with kidney or liver issues.
- Be aware of hypoglycemia symptoms, and always have a plan to treat lows.
- People with G6PD deficiency need special monitoring due to hemolytic anemia risk.
- Compared with some older sulfonylureas, it offers less weight gain, lower hypoglycemia risk, and better cardiac safety.
Most importantly, you do not need to make these decisions alone. Partner closely with your healthcare team. Share your readings, your concerns, and your daily realities. Together, you can find a dose and regimen that supports both safer use and better quality of life 🌿.
This article was structured with Rank Math SEO optimization in mind to keep it easy to read and revisit, but your personal care plan should always be guided by a qualified professional who knows your full medical picture.

1 Comment
Pingback: How Long Does Alcohol Stay in Urine: 7 Shocking Facts You Need to Know