


Job Title: Oncologist & Cancer Research Specialist
Institutional Affiliation: Sun Yat-sen University Cancer Center (Guangzhou, China)
Specialties: Clinical Oncology | Cancer Prevention Strategies | Oncological Research Insights
Dr. Yichen Xu is a dedicated Oncologist and cancer research specialist with an extensive background in clinical oncology. At Healthy Post, Dr. Xu is committed to directly authoring evidence-based health journalism, ensuring all medical content meets the highest standards of clinical accuracy, contemporary medical consensus, and trustworthiness.
Verify Medical Credentials:
Medical Accuracy Verified
This article has been written and clinically verified by Dr. Yichen Xu, a specialist in Medical Oncology.
Medical Disclaimer: The content on Healthy Post is for educational and informational purposes only and does not substitute for professional medical advice, diagnosis, or treatment. While evaluating breast size and cancer risk is an important aspect of patient awareness, clinical data shows that high mammographic breast density (the ratio of glandular tissue to fat) is a significantly stronger independent risk factor than physical breast volume alone. Furthermore, dense tissue can mask lesions on standard imaging. Always consult a qualified medical oncologist, radiologist, or primary healthcare provider for regular clinical breast exams, personalized risk assessments, and routine screening mammograms.
Many people worry about breast size and cancer risk. It is an understandable fear. Breast shape, cup size, and body changes are visible. Internal tissue composition is not. In our medical editorial work, we often see this exact concern come up after a mammogram, during a routine exam, or even after someone hears a family story about breast cancer.
Here is the short answer: external breast size does not, by itself, determine breast cancer risk. What matters far more is what the breast is made of on the inside, especially mammographic breast density. That distinction helps answer another common question: does breast size affect cancer risk? Most studies say not in a direct, independent way. Instead, doctors pay much closer attention to density, age, genetics, hormone exposure, and overall risk profile.
Understanding that difference can lower anxiety and lead to smarter screening decisions. It also helps separate internet myths from the evidence.
If you are trying to make sense of breast health alongside other cancer concerns, readers often also explore Endometrial Cancer Staging Symptoms or Five major signs of early colorectal cancer when looking at broader screening awareness.
1. Breast size and cancer risk are not the same thing
The most important point is simple. Breast size and cancer risk are not interchangeable.
Breast size usually reflects:
- overall body frame
- the amount of adipose tissue volume (breast fat cells)
- genetics
- hormonal changes across life
- weight fluctuations
- pregnancy and breastfeeding history
Cancer risk, on the other hand, is shaped by a different set of factors:
- age
- family history
- BRCA1 and BRCA2 genetic mutations
- other high-penetrance germline mutations
- breast density
- reproductive history
- alcohol use
- hormone exposure
- prior chest radiation
- certain biopsy findings
A larger bra cup does not automatically mean more dangerous tissue. Many larger breasts contain more fatty tissue, not more high-risk tissue. Fatty breasts can actually be easier to read on mammograms because fat appears dark on imaging, while many tumors appear white and stand out more clearly.
That is why the question does breast size affect cancer risk needs a careful answer. Physical volume alone is not the driver. Internal tissue pattern is.
2. The inside of the breast matters more than the outside
Breasts are made up of a mix of:
- fat tissue
- connective tissue
- milk ducts and lobules
- glandular epithelium
- blood vessels and lymphatic structures
This is where the real story begins.
When radiologists talk about “dense breasts,” they are not describing how breasts feel by hand. They are talking about what shows up on a mammogram. Dense breasts have more fibroglandular tissue and less fat. That matters for two reasons.
First, dense tissue is associated with a higher risk of breast cancer.
Second, dense tissue can hide tumors on standard mammograms.
This is the central issue in the debate around breast size and cancer risk. A person with small breasts may have very dense tissue and therefore a higher screening challenge. A person with larger breasts may have mostly fatty tissue and no density-related masking problem.
3. Dense breasts vs fatty breasts: why this difference matters
The phrase dense breasts vs fatty breasts is one of the most useful comparisons for patients.
Here is the practical difference:
| Breast Type | Main Tissue Makeup | Mammogram Appearance | Cancer Visibility on Mammogram | Relative Risk Consideration |
|---|---|---|---|---|
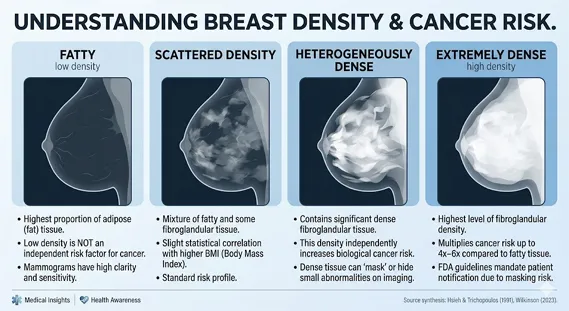
| Almost entirely fatty | Mostly fat | Dark | Tumors often easier to spot | Generally lower density-related risk |
| Scattered fibroglandular density | Mostly fat with some dense tissue | Mostly dark with some white areas | Usually still readable | Common and often manageable |
| Heterogeneously dense | More dense tissue | More white areas | Small masses may be hidden | Elevated risk and masking concern |
| Extremely dense | Predominantly dense fibroglandular tissue | Large white areas | Significant masking effect | Higher risk and lower mammographic sensitivity |
Radiologists usually classify density using BI-RADS categories:
- A: almost entirely fatty
- B: scattered fibroglandular densities
- C: heterogeneously dense
- D: extremely dense
Categories C and D are the ones that usually trigger more discussion.
This is why dense breasts vs fatty breasts is much more clinically meaningful than cup size. In dense tissue, both the tissue and many cancers can appear white on a mammogram. It becomes a white-on-white problem.
4. What causes high breast density?
Patients often ask what causes high breast density, especially after a first screening notice. The answer is not always one single cause. Density is influenced by a mix of biology, life stage, and hormones.
Common factors linked to higher density include:
- younger age
- premenopausal status
- genetics and family patterns
- lower body fat in some individuals
- hormone replacement therapy
- certain hormonal exposures
- lower parity in some populations
Aging often reduces density, especially after menopause, when breasts commonly undergo fatty involution. But that is not universal. Some postmenopausal women still have dense breasts.
Research also suggests roles for:
- circulating endogenous estrogen
- reproductive history
- alcohol intake
- ethnic and population differences
So, what causes high breast density? In plain language: hormones, genetics, and life stage are major contributors. Lifestyle may play a supporting role, but density is not something a person can fully control.
5. Why density raises risk in two different ways
High breast density matters because it creates a double challenge.
A. It is linked with higher biological risk
Most studies agree that extremely dense breasts are associated with a higher breast cancer risk compared with breasts that are mostly fatty. Older landmark studies found risk increases in the range of four to six times in some comparisons.
Scientists are still studying why. One theory is that more fibroglandular tissue means more active tissue environment, including stromal and epithelial components, where malignant changes may arise. This may be more relevant than simple physical size.
B. It can hide early cancers
This masking effect is a major issue. Standard 2D mammography becomes less sensitive in extremely dense breasts. That means cancer can be present but less visible.
That is why the question is not only does breast size affect cancer risk, but also: what kind of tissue is present, and how well can we see through it?
For some patients, this leads to discussion of supplemental screening tools (ultrasound or breast MRI) or digital breast tomosynthesis (3D mammography).
6. The FDA breast density rule changed the conversation
A major recent shift came from the U.S. Food and Drug Administration. Under national mammography reporting rules, patients must now be informed about their breast density in clearer language.
That matters because people can finally act on information they may not have previously received.
In practice, this means your mammogram report may mention whether your breasts are:
- almost entirely fatty
- scattered in density
- heterogeneously dense
- extremely dense
This is not meant to alarm you. It is meant to inform you.
If your report shows dense tissue, it is reasonable to ask:
- Do I need digital breast tomosynthesis (3D mammography) next time?
- Would supplemental screening tools (ultrasound or breast MRI) help in my situation?
- What is my overall risk when family history and genetics are included?
- Should I see a breast specialist or high-risk clinic?
For U.S. readers, the FDA’s breast density notification guidance is an important reference: FDA mammography information.
7. Myths that keep confusing people
Several myths continue to blur the real conversation about breast size and cancer risk.
Myth 1: Larger breasts automatically mean higher cancer risk
Not true. Larger breasts may simply contain more fat. Fat alone does not equal higher breast cancer risk in the same way dense tissue does.
Myth 2: Small breasts are safer
Also not necessarily true. A smaller breast can still be very dense. Density, not external size, is often the more relevant concern.
Myth 3: Underwire bras cause cancer
There is no good evidence that underwire bras cause breast cancer by blocking lymphatic flow.
Myth 4: You can tell breast density by touch
You cannot. Density is a radiology finding, not a tactile one.
This is where patient education matters most. A person can appear “low risk” based on myths and still have dense breast tissue that deserves a more tailored screening conversation.
8. Other risk factors matter more than volume alone
When we review risk profiles, breast size is rarely the headline issue. These factors deserve more attention:
- family history of breast or ovarian cancer
- inherited mutations such as BRCA1 and BRCA2 genetic mutations
- other high-penetrance germline mutations
- prior atypical hyperplasia or certain biopsy findings
- age at first period and menopause
- hormone replacement therapy
- alcohol intake
- obesity after menopause
- prior chest radiation
- history of hormone receptor-positive cancers in family context
If you are already navigating treatment questions in another area, you may also find Cancer Patient Diet & Side Effect Management useful, especially when cancer prevention and survivorship topics overlap.
For evidence-based risk information, the CDC breast cancer risk factors page offers a reliable overview.
9. A lesser-known angle: the left-side laterality phenomenon
One of the more fascinating details in the research is the left-side laterality phenomenon (the clinical asymmetry angle). Breast cancer has been observed slightly more often in the left breast than the right in several studies and meta-analyses.
Why would that happen? No one has a complete answer. Proposed explanations include:
- subtle anatomical asymmetry
- the left breast often being slightly larger on average
- developmental patterns
- environmental or behavioral influences
- even handedness-related theories
This does not mean a larger left breast causes cancer. It simply highlights how complex the relationship is between anatomy and disease. Once again, size alone is too crude a measure. Internal biology matters more.
This kind of nuance is often missing from simplified discussions of breast size and cancer risk.

10. What should you do if you have dense breasts?
If you learn you have dense breasts, the next step is not panic. It is context.
Ask your clinician:
- What BI-RADS density category do I have?
- Do I have other risk factors besides density?
- Is digital breast tomosynthesis (3D mammography) available to me?
- Would supplemental screening tools (ultrasound or breast MRI) be appropriate?
- Should I consider formal risk assessment or genetic counseling?
This is especially important if you also have:
- a strong family history
- prior high-risk biopsy findings
- known genetic mutations
- persistent breast symptoms
- prior chest radiation
You may also want to review trusted guidance from NHS breast cancer symptoms if you are sorting out symptom awareness alongside screening results.
11. Breast reduction, body size, and screening reality
Another overlooked angle is breast reduction surgery. For some people with very large breasts, reduction surgery can improve comfort and may change how future imaging looks. It can sometimes reduce overlapping tissue shadows and make exams easier to interpret, although postsurgical scarring can also create its own imaging considerations.
This is not a cancer prevention strategy in the routine sense. It is a structural and quality-of-life decision with screening implications.
It is also worth acknowledging a real care gap. Patients in larger bodies are sometimes told, too casually, that large breasts mean higher risk. That can be misleading. At the same time, the more important issue of density may receive less attention. Better care means looking beyond assumptions and focusing on actual risk markers.
If you are comparing symptoms across cancer types, some readers also explore Is Low Potassium a Sign of Cancer? when trying to understand which signs are meaningful and which are indirect.
FAQs
Does breast size affect cancer risk?
Not directly in an independent way. Current evidence suggests outer breast size alone is not a reliable predictor of risk. Breast density, genetics, age, and hormone-related factors matter more.
Dense breasts vs fatty breasts: which is riskier?
In general, dense breasts carry more concern because they are linked with higher risk and can make tumors harder to see on mammograms. Fatty breasts are usually easier to image.
What causes high breast density?
Common factors include genetics, younger age, premenopausal status, hormone replacement therapy, and natural hormonal environment. For many people, there is no single cause.
Can large breasts make mammograms harder?
They can sometimes make positioning more technically challenging, but size is not the same as density. The bigger issue is whether the tissue is dense or fatty.
Should I ask for ultrasound or MRI if I have dense breasts?
Maybe. This depends on your overall risk. Some people benefit from supplemental screening tools (ultrasound or breast MRI), especially when dense tissue is combined with other risk factors.
Do dense breasts mean I will get cancer?
No. Dense tissue increases risk and may reduce mammogram sensitivity, but it does not mean cancer is inevitable. It means screening discussions should be more personalized.
Conclusion
The best way to understand breast size and cancer risk is to separate visible anatomy from internal tissue biology. Cup size is not the key predictor many people think it is. Breast density is far more important. That is why questions like does breast size affect cancer risk, dense breasts vs fatty breasts, and what causes high breast density all lead back to the same lesson: screening quality and tissue composition matter more than appearance.
If your mammogram mentions dense tissue, use that information. Ask questions. Review your family history. Discuss whether digital breast tomosynthesis (3D mammography) or other screening options make sense for you. And if you are building a broader cancer-awareness plan, resources like Cancer Patient Diet & Side Effect Management, Endometrial Cancer Staging Symptoms, and Five major signs of early colorectal cancer can help you think more comprehensively about prevention, symptoms, and follow-up care.
This article is informational and should support, not replace, medical advice from your own clinician.
References
- Boyd NF, et al. Mammographic densities and breast cancer risk. Cancer Epidemiology, Biomarkers & Prevention. 1998.
- Nazari SSM, Mukherjee P. An overview of mammographic density and its association with breast cancer. Breast Cancer. 2018.
- FDA. Mammography Quality Standards Act and Program.
- CDC. Breast cancer risk factors.
- NHS. Breast cancer symptoms.
2 Comments
Pingback: Atypical Ductal Hyperplasia Core Needle Biopsy: Understanding Your Upgrade Risk
Pingback: How to Manage Chemotherapy Side Effects at Home | Complete Patient Guide