

Expert Medical Authorship & Verification
This article was written and clinically verified by Dr. Liping Shen, a specialist in Gynecologic Oncology. The information provided is for educational purposes only and is not intended to replace professional medical advice, diagnosis, or treatment. Atypical ductal hyperplasia and related breast conditions can vary significantly between individuals.
Medical Disclaimer: Always seek the guidance of your physician or another qualified healthcare provider with any questions you may have regarding a medical condition, biopsy results, or treatment options. Never disregard professional medical advice or delay seeking it because of something you have read here.
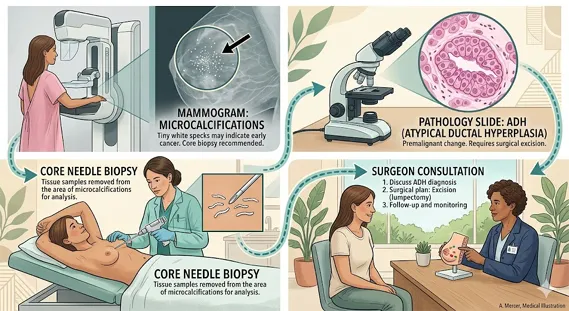
Hearing that your atypical ductal hyperplasia core needle biopsy showed an abnormal result can feel unsettling. We see this often in clinical education work. A patient goes in for follow-up imaging after abnormal mammogram calcifications, expects a routine answer, and instead hears the term “high-risk breast lesion.” That moment brings understandable questions. Is this cancer? How worried should I be? What happens next?
The short answer is this: atypical ductal hyperplasia, or ADH, is not breast cancer. But it is not a finding doctors ignore. It sits in an important middle ground. It is a benign lesion with features that overlap with Ductal carcinoma in situ (DCIS), and that overlap helps explain why the ADH breast biopsy upgrade rate matters so much after a core needle biopsy.
Most studies agree on two key points. First, ADH raises future breast cancer risk compared with the general population. Second, when ADH is found on a core needle biopsy, surgical excision is often recommended because a larger tissue sample may reveal DCIS or invasive cancer that the needle sample did not catch. That possibility is what clinicians mean by “upgrade risk.”
In this guide, we will walk through what ADH means, why the biopsy result can be confusing, how doctors estimate risk, and what treatment and follow-up may look like. We will also touch on related concerns, including can breast hyperplasia turn into cancer, atypical ductal hyperplasia vs DCIS, and how family history changes the discussion. If you are also exploring broader breast health topics, articles such as Family History and Breast Cancer and What to do if you get breast cancer can help place this diagnosis in context.
1. What is atypical ductal hyperplasia?
Atypical ductal hyperplasia is an overgrowth of abnormal-looking cells inside the milk ducts of the breast. Under the microscope, the cells are more crowded and more patterned than normal duct cells. But they do not fully meet the criteria for cancer.
That distinction matters.
ADH is considered:
- Benign, not cancer
- A marker of increased future breast cancer risk
- A lesion that can resemble low-grade DCIS on small samples
- A finding that often needs more tissue evaluation
In practice, the challenge is not just what ADH is. It is what it may be sitting next to. A core biopsy samples only part of the area seen on imaging. If that area contains a mix of ADH and a nearby cancer focus, the needle may capture only the atypical portion.
That is why the phrase atypical ductal hyperplasia vs DCIS comes up so often. On a spectrum of duct cell changes, ADH and DCIS can look similar, but DCIS is more extensive and is classified as stage 0 breast cancer.
2. Why is ADH often found on a core needle biopsy?
ADH is usually not something a person feels as a lump. It is often discovered after screening.
Common reasons a biopsy is ordered include:
- Clusters of abnormal mammogram calcifications
- A small imaging abnormality on mammogram or ultrasound
- A suspicious area that needs tissue diagnosis
- Follow-up of a screening finding in higher-risk patients
A core needle biopsy uses a hollow needle to remove several tissue samples. It is less invasive than surgery and is a standard first step in breast diagnosis. From the pathology side, the biopsy can identify a high-risk lesion, but it may not show the full picture.
This is where Radiologic-pathologic correlation becomes essential. That means the radiologist and pathologist compare what was seen on imaging with what was found under the microscope. If the pathology result does not fully explain the imaging concern, the chance of an upgrade may be higher.
For example, if imaging shows a suspicious cluster of calcifications but the biopsy finds only a very small focus of ADH, the team may worry that the sample underrepresented the lesion.
3. What does “upgrade risk” mean after an ADH diagnosis?
Upgrade risk means the chance that surgical excision will find a more serious diagnosis than the core biopsy showed. Usually that means Ductal carcinoma in situ (DCIS) or invasive breast cancer.
This is the heart of the ADH breast biopsy upgrade rate discussion.
Across studies, the upgrade rate after excision often falls in the 10% to 30% range. The exact number depends on:
- The size of the lesion
- How much ADH is present in the biopsy
- Whether calcifications were fully sampled
- Imaging-pathology agreement
- Needle type and number of samples taken
- Patient-specific risk factors
Here is a simple comparison:
| Finding | What it means | Cancer? | Usual next step |
|---|---|---|---|
| ADH | Abnormal duct cells, limited in extent | No | Often surgical excision |
| DCIS | Cancer cells confined to milk ducts | Yes, stage 0 | Surgery and tailored treatment |
| Invasive breast cancer | Cancer has spread beyond the duct wall | Yes | Multidisciplinary treatment |
Most studies agree that excision is especially important when there is radiologic-pathologic discordance, a larger area of calcifications, or limited biopsy sampling.
A patient once described this well during a clinic education session: “So the biopsy is like reading one page of a book, and surgery helps read the whole chapter.” That is not a perfect analogy, but it captures the issue.
4. Atypical ductal hyperplasia vs DCIS: why the distinction is difficult
The phrase atypical ductal hyperplasia vs DCIS is not just a patient question. It is also a pathology challenge in some cases.
Both conditions can involve:
- Similar-looking abnormal duct cells
- Low-grade cellular changes
- Associations with calcifications on mammography
The key differences are usually based on:
- Extent of the abnormal cell growth
- Degree of architectural involvement
- Number of duct spaces affected
- Overall pattern seen in a larger tissue sample
In plain language, ADH is smaller and more limited. DCIS is more developed and more widespread within the ducts.
This matters because treatment paths differ. ADH is not treated as cancer, but it is treated seriously because of both future risk and the chance that the original needle sample underestimated the lesion.
A related lesion you may hear about is Atypical lobular hyperplasia (ALH). ALH also increases breast cancer risk, but it arises in the lobules rather than the ducts. The management discussion can differ, though both lesions are considered markers of elevated risk.
5. Can breast hyperplasia turn into cancer?
This is one of the most common patient questions: can breast hyperplasia turn into cancer?
The safest answer is nuanced. ADH itself is not cancer. But it is associated with a higher likelihood of developing breast cancer over time, and it can be found near areas of DCIS or invasive cancer. So it is better understood as both a risk marker and, in some cases, part of a pathway of abnormal cellular change.
Long-term research suggests that women with ADH have about a 4- to 5-fold increased risk of future breast cancer compared with the general population. Some studies estimate the cumulative risk roughly as:
- About 7% at 5 years
- About 13% at 10 years
- Around 30% at 25 years
These numbers vary between studies and populations, but the trend is consistent. Risk persists over time.
That does not mean every person with ADH will develop breast cancer. Far from it. It means follow-up matters. Your personal risk also depends on age, family history, breast density, genetic factors, and prior breast lesions.
If you are trying to understand how inherited risk fits in, Family History and Breast Cancer is a useful related topic to review alongside an ADH diagnosis.
6. Why doctors often recommend surgical excision
When ADH appears on a core biopsy, many breast specialists recommend a surgical excision, sometimes called an excisional biopsy or lumpectomy of the area. The goal is diagnostic clarity.
Reasons include:
- Core biopsy samples only part of the lesion
- The ADH breast biopsy upgrade rate is clinically meaningful
- ADH can sit next to DCIS or invasive cancer
- Imaging and pathology may not perfectly match
- Management becomes safer when the full lesion is assessed
Current practice patterns are influenced by breast surgery and pathology guidelines, including recommendations from organizations such as the American Society of Breast Surgeons. In our review of patient education pathways, the most consistent message is this: excision is often advised when confidence in the sampling is limited or when the lesion appears higher risk on imaging.
That said, not every case is identical. In selected low-risk situations, some teams may discuss close imaging surveillance instead of immediate surgery. This is usually considered only when the lesion is very small, imaging-pathology findings are strongly concordant, and sampling appears thorough.
7. What treatment and follow-up may look like after excision
If excision shows only ADH and no cancer, treatment usually shifts toward risk reduction and surveillance rather than cancer therapy.
A typical follow-up plan may include:
- Annual mammograms
- Clinical breast exams every 6 to 12 months
- Breast MRI in selected high-risk patients
- Lifestyle changes that may help lower risk
- Discussion of preventive medication
Risk-reducing medication is an important option for some patients. These drugs include Selective Estrogen Receptor Modulators (SERMs) such as tamoxifen and raloxifene, as well as aromatase inhibitors like anastrozole or exemestane in appropriate patients.
These medications do not fit everyone. Benefits, side effects, menopausal status, and clotting history all matter. But they can significantly reduce future breast cancer risk in the right clinical setting.
Lifestyle steps may also help:
- Maintain a healthy weight
- Exercise regularly
- Limit alcohol
- Avoid smoking
- Keep up with recommended screening
Patients sometimes ask whether body type changes risk. That opens the door to broader breast health discussions, including Breast Size and Cancer Risk, though breast size alone does not determine whether someone will develop ADH or breast cancer.

8. What newer research is showing
Recent research has added more detail to how ADH behaves biologically. Molecular studies suggest that some ADH lesions share genetic alterations seen in low-grade DCIS. That does not mean all ADH becomes cancer. It does reinforce why careful follow-up is justified.
From a global perspective, management also depends on healthcare access. In some regions, including parts of South Asia, breast MRI may not be widely available or affordable. In those settings, mammography, pathology review, and excision remain especially important.
This is also where trust in the care pathway matters. Patients benefit when radiologists, pathologists, surgeons, and primary care clinicians are all aligned. Good care is rarely one opinion in isolation. It is a coordinated process.
9. Practical questions to ask your doctor
If your biopsy shows ADH, these questions can help:
- Do my imaging and pathology results match?
- What is my estimated upgrade risk?
- Was the area fully sampled on biopsy?
- Do you recommend surgical excision, and why?
- Should I consider MRI or genetic counseling?
- Am I a candidate for tamoxifen or other preventive therapy?
If your diagnosis later changes to cancer, practical planning becomes the next step. At that point, resources like What to do if you get breast cancer may help you prepare for treatment discussions. And for patients navigating reconstruction concerns further down the line, How much do you know about breast plastic surgery can be a useful educational companion.
FAQs
Is atypical ductal hyperplasia a cancer diagnosis?
No. ADH is not cancer. It is a benign but high-risk breast lesion associated with a higher future risk of breast cancer and a possible upgrade at excision.
What is the ADH breast biopsy upgrade rate?
Published studies often report an ADH breast biopsy upgrade rate of about 10% to 30% after surgical excision, though the exact rate depends on sampling quality and imaging findings.
Can breast hyperplasia turn into cancer?
When patients ask, can breast hyperplasia turn into cancer, the answer is that ADH itself is not cancer, but it is linked to increased future risk and may be found near DCIS or invasive disease.
How is atypical ductal hyperplasia vs DCIS different?
In atypical ductal hyperplasia vs DCIS, the main difference is extent. ADH is limited and benign. DCIS is more extensive and is considered stage 0 breast cancer.
Do I always need surgery after ADH on core biopsy?
Not always, but often. Many clinicians recommend excision because a core biopsy may miss nearby cancer. The decision depends on Radiologic-pathologic correlation, lesion size, and individual risk.
Should I worry more if I have a family history?
Family history can increase overall breast cancer risk and may affect screening and prevention recommendations. This is why related education such as Family History and Breast Cancer can be helpful.
Conclusion
An atypical ductal hyperplasia core needle biopsy result can be frightening at first glance, but it is best understood as a warning sign, not a final cancer diagnosis. ADH is benign. Still, it deserves careful attention because the ADH breast biopsy upgrade rate is high enough that many patients are advised to have surgical excision. The concern is not only what the biopsy showed, but what it may have missed.
Most studies agree that ADH increases long-term breast cancer risk, which is why surveillance, prevention, and personalized follow-up matter. If you are weighing questions like can breast hyperplasia turn into cancer or trying to understand atypical ductal hyperplasia vs DCIS, the most helpful next step is a detailed conversation with your breast care team. Ask about imaging-pathology concordance, your personal risk factors, and whether preventive therapy makes sense for you.
A measured, informed plan is the goal. Not panic. Not delay. Just the right next step, based on the best evidence available.